Effect of Zhikang Capsule Assisted LEEP on Postoperative Recovery Speed and the Incidence of Complications of Patients with Cervical Intraepithelial Neoplasia
Chen Chen1, Hongfeng Zhang1*
1Department of Scientific Research, Handan Central Hospital, Handan, Hebei Province, China
*Correspondence to: Hongfeng Zhang, Department of Scientific Research, Handan Central Hospital, Handan 057150, Hebei Province, China; Email:1388097@163.com
Abstract
Objective: To investigate the role of Zhikang capsule assisted loop electrosurgical excision procedure (LEEP) operation for intervening cervical intraepithelial neoplasia (CIN) on improving the recovery speed and reducing the incidence of complications.
Methods: Altogether 91 CIN patients in our hospital were selected as the research participants. Patients treated with Zhikang capsule assisted LEEP operation were the research group (RG) (48 cases), and patients treated with LEEP operation were the control group (CG) (43 cases). The related indexes and incidence of postoperative complications between the CG and the RG were compared. Inflammatory reaction, immune function, psychological status score, total bleeding, hospital stay and quality of life were evaluated.
Results: The drainage time, bleeding time and wound healing time in the RG were shorter than those in the CG (P<0.05). The incidence of complications in the RG was evidently lower than that in the CG (P=0.034). IL-4 in the RG was evidently lower than that in the CG (P<0.05), while IFN-γ and IL-2 were evidently higher than those in the CG (P<0.05). CD3+ and CD4+ in the RG were evidently higher than those in the CG (P<0.05), while CD8+ in the RG were evidently lower than those in the CG (P<0.05). After intervention, SDS and SAS scores in the RG were evidently lower than those in the CG (P<0.05). The total bleeding and hospital stay in the RG were less than those in the CG (P<0.05). The quality of life in the RG was better than that in the CG (P<0.05).
Conclusion: Zhikang capsule assisted LEEP operation can effectively improve the recovery rate of patients and reduce the incidence of complications, which is worthy of clinical application.
Keywords: Zhikang capsule, LEEP operation, cervical intraepithelial neoplasia
1 Introduction
Cervical carcinoma is a serious global public health problem[1]. Data have shown that cervical carcinoma cases in China account for 14% of new cervical carcinoma cases in the world[2]. Smoking, multiple sexual partners, premature sexual life, multiple pregnancies and multiple births are the risk factors of cervical carcinoma, and HPV infection is considered to be the main cause of cervical carcinoma[3]. Relevant literature pointed out that HPV infection is closely related to high risk of cervical intraepithelial neoplasia (CIN)[4]. CIN is a precarcinomaous lesion of cervical carcinoma, in which the cervical epithelium is replaced by cells with different degrees of atypia[5]. It can be confirmed histologically from biopsy samples and can be divided into three stages (1, 2 and 3)[6]. It is estimated that CIN can persist or develop into cervical carcinoma after 10-20 years in 70% of women with diseases[7]. With the continuous development of medical examination, cervical carcinoma screening tools are widely used in clinic, and the detection rate of CIN is also elevating[8]. Therefore, in order to better prevent cervical carcinoma and reduce the incidence, the clinical treatment of CIN is needed exploration.
Loop electrosurgical excision procedure (LEEP) is currently the primary treatment method for CIN[9]. The high-frequency radio knife is applied to generate microwaves from the tip of the electrode through the LOOP wire, so that the moisture in the cell forms steam waves to complete the surgical purposes such as cutting and hemostasis[10]. According to previous data, LEEP has good curative effect, little pain and short operation time, and can also keep complete and continuous specimens for pathological examination[11]. However, it takes 2-3 months for the wound to heal after LEEP operation[12]. During this period, if the patient does not follow the doctor's advice and has sexual life, it may cause vaginal inflammation, thus affecting the repair of normal cervical tissue[13]. Many studies have found that Zhikang capsule can effectively reduce postoperative wound bleeding and accelerate wound healing, which is conducive to postoperative recovery[14]. However, the value of LEEP in CIN surgery is still lack of sufficient data support. Therefore, this study focused on the effect of Zhikang capsule assisted LEEP intervention on the postoperative recovery speed and complication rate of CIN patients, and provided reliable ideas and methods for improving the postoperative recovery of CIN in the future.
2 Materials and methods
2.1 General Information
Altogether 91 CIN patients admitted to our hospital from April 2017 to June 2019 were selected as the research participants. Patients with LEEP operation assisted by Zhikang Capsule were collected as the research group (RG) (48 cases) and patients with LEEP operation intervention as the control group (CG) (43 cases). The experiment has been approved by the Ethics Committee of our hospital.
2.2 Inclusion and Exclusion Criteria
Inclusion criteria: All the patients were confirmed as CIN by gynecological examination, cervical cytology and HPV virus examination, colposcopy and histopathological examination; all the patients were confirmed as grade I and grade II of CIN; all the patients were married women of childbearing age; patients had complete case data; patients agreed to participate in this experiment.
Exclusion criteria: patients during pregnancy and lactation; patients with abnormal immune function and coagulation function; patients with contraindications of LEEP operation; patients had other major diseases; patients were transferred form the other hospital or did not cooperate with treatment.
2.3 Method
The CG was treated with LEEP. All patients underwent surgery during non-menstrual period. Firstly, cervical disinfection and local anesthesia were performed. The local lesion was excised by using the suitable coil, with the excising range of 3-5mm from the outer edge of the lesion and with the depth of 10-20mm. The ring electrode was used for electrocoagulation to stop bleeding, and the tissue was excised for pathological examination. After the operation, the wound of the patients were compressed to stop bleeding, antibiotics were used, and sexual life was forbidden.
RG: On the basis of the CG, Zhikang capsule was used as an auxiliary intervention, and Zhikang capsule powder was applied to the wound. Then, the gauze was filled in the wound, taken out 24h after operation, and then applied continuously for one week, 0.9g/time, 3 times/day. Sexual life was forbidden after operation, and antibiotics were taken by patients orally.
2.4 Outcome Measures
Main outcome measures: Postoperative related indexes of two groups: drainage time, bleeding time and wound healing time; incidence of postoperative complications in two groups; psychological status scores before and after intervention in the two groups; quality of life of patients in two groups after operation.
Secondary observation indexes: the levels of interleukin-4 (IL-4), interferon-γ (IFN-γ) and interleukin-2 (IL-2) in two groups after operation (ELISA detection); CD3+, CD4+ and CD8+ in two groups after operation (flow cytometry); total bleeding and hospital stay of two groups.
2.5 Detection Method
Serum levels of IL-4, IFN-γ and IL-2 were detected using ELISA. Blank well, standard well and sample well to be tested were set. SO standard with concentration of 0 was added into the blank well, 50µL of standard with different concentrations was added into the standard well, and 10µL of sample to be tested was added into the sample well, then 40µL of sample diluent was added to each well, except the blank well. A total of 100µL of HRP-labeled detection antibody was added to the standard well and the sample well. The reaction wells were sealed with a sealing membrane, incubated in a water bath at 37℃ for 65min. The liquid was then discarded, the wells were dried on an absorbent paper, filled with washing liquid, and placed for 2min. After that, the washing liquid was discarded, the wells were dried with an absorbent paper, for a total of 6 times. A 50µL of substrate was added to each well, and incubated in dark at 37℃ for 10min. A 50µL stopping solution was added to each well, and the OD value of each well at 450nm within 15min was measured.
2.6 Statistical Analysis
SPSS22.0 was applied to process the data results, and Graphpad7 to visualize the data results. Counting data were expressed in (rate) and compared by Chi-square test. Measurement data were expressed as mean±SD, and the data conforming to normal distribution was tested by t. Rank sum test was applied for data conforming to non-normal distribution. P<0.05, the difference was statistically significant.
3 Results
3.1 General Information of Patients
There were no statistical differences in general data such as age, BMI, CIN grade, residence, educational level, family history, smoking history, drinking history, marital status, and nationality between the CG and the RG (P>0.05), as shown in Table 1.
Table 1. General Data [n(%)]
|
RG (n=48) |
CG (n=43) |
t or 2 |
P |
Age (years) |
35.57±5.6 |
34.82±5.8 |
0.627 |
0.532 |
BMI (kg/cm2) |
24.32±3.06 |
24.46±4.12 |
0.185 |
0.854 |
CIN grading |
|
|
0.033 |
0.856 |
I |
27 (56.25) |
25 (58.14) |
|
|
II |
21 (43.75) |
18 (41.86) |
|
|
Residence |
|
|
0.026 |
0.871 |
Urban |
35 (72.92) |
32 (74.42) |
|
|
Rural |
13 (27.08) |
11 (25.58) |
|
|
Educational level |
|
|
0.136 |
0.713 |
<high school |
15 (31.25) |
15 (34.88) |
|
|
≥high school |
33 (68.75) |
28 (65.12) |
|
|
Family history |
|
|
0.096 |
0.757 |
Yes |
9 (18.75) |
7 (16.28) |
|
|
No |
39 (81.25) |
36 (83.72) |
|
|
Smoking history |
|
|
0.083 |
0.774 |
Yes |
17 (35.42) |
14 (32.56) |
|
|
No |
31 (64.58) |
29 (67.44) |
|
|
Drinking history |
|
|
0.145 |
0.703 |
Yes |
26 (54.17) |
25 (58.14) |
|
|
No |
22 (45.83) |
18 (41.86) |
|
|
Marital status |
|
|
0.212 |
0.646 |
Married |
36 (75.00) |
34 (79.07) |
|
|
Divorced |
12 (25.00) |
9 (20.93) |
|
|
Nationality |
|
|
0.271 |
0.602 |
Han |
40 (83.33) |
34 (79.07) |
|
|
Minorities |
8 (16.67) |
9 (20.93) |
|
|
3.2 Comparison of Postoperative Related Indexes between the CG and the RG
The related indexes such as drainage time, bleeding time and wound healing time were compared between the CG and the RG. As shown in Figure 1, those indexes of the RG were all smaller than those of the CG (P<0.05).
|
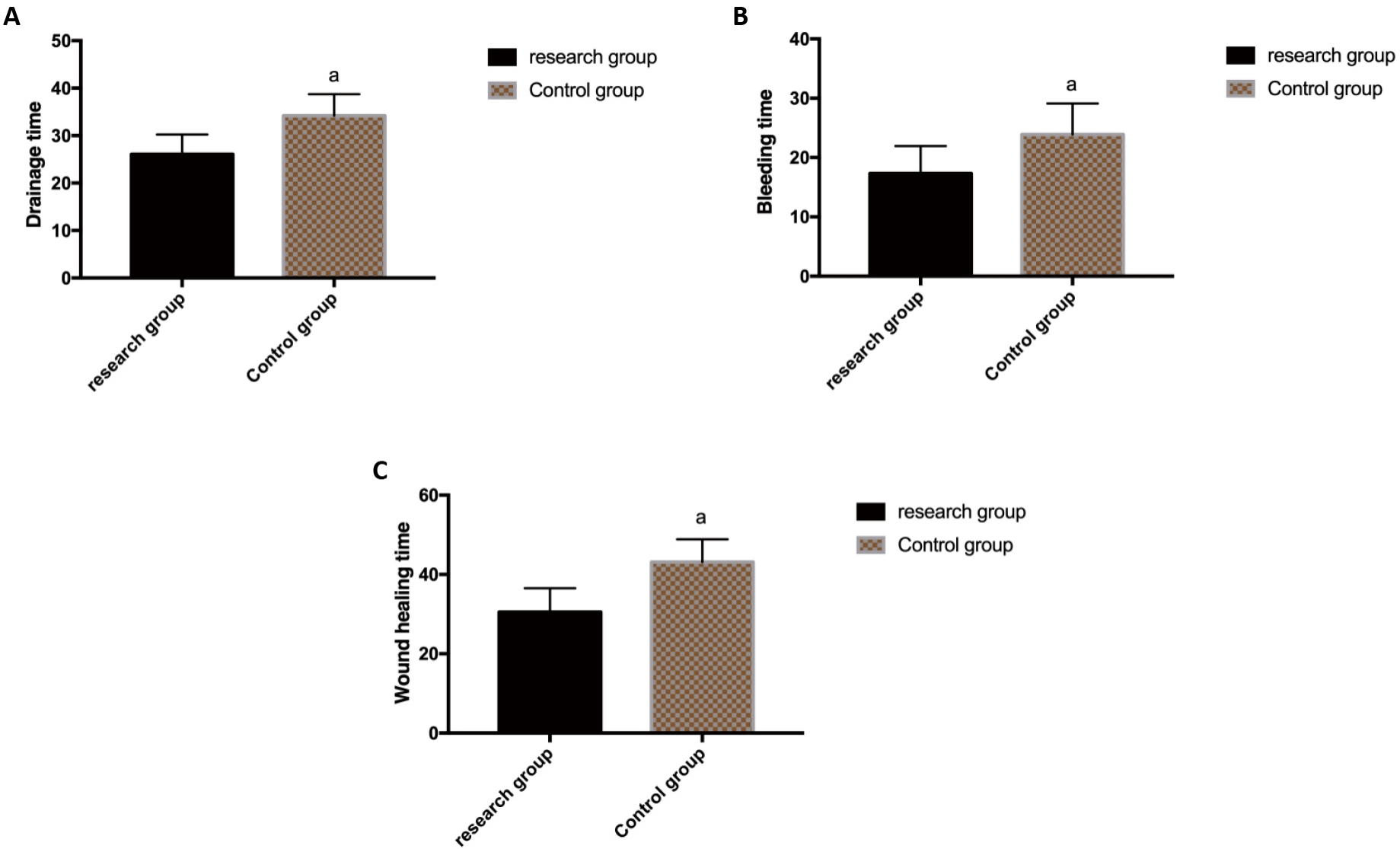
Figure 1. Comparison of postoperative related indexes between the CG and the RG. A: Postoperative drainage time of two groups of patients; B: Postoperative bleeding time of two groups of patients; C: Postoperative wound healing time of two groups of patients. Note: aP<0.05.
3.3 Incidence of Postoperative Complications
The total incidence of postoperative complications in the RG (2.08%) was evidently lower than that in the CG (13.95%) (P=0.034), as shown in Table 2.
Table 2. Incidence of Complications in Two Groups [n(%)]
|
RG (n=48) |
CG (n=43) |
2 |
P |
Cervical infection |
1 (2.08) |
4 (6.98) |
|
|
Cervical eversion |
0 (0.00) |
1 (2.33) |
|
|
Postoperative bleeding |
0 (0.00) |
0 (0.00) |
|
|
Adhesion of cervical orifice |
0 (0.00) |
1 (2.33) |
|
|
Total |
1 (2.08) |
6 (13.95) |
4.501 |
0.034 |
3.4 Comparison of IL-4, IFN-γ and IL-2 Levels between the CG and the RG after Operation
The levels of IL-4, IFN-γ and IL-2 in the CG and the RG were detected and compared. As shown in Figure 2, IL-4 in the RG were evidently lower than those in the CG (P<0.05), while IFN-γ and IL-2 were evidently higher than those in the CG (P<0.05).
|
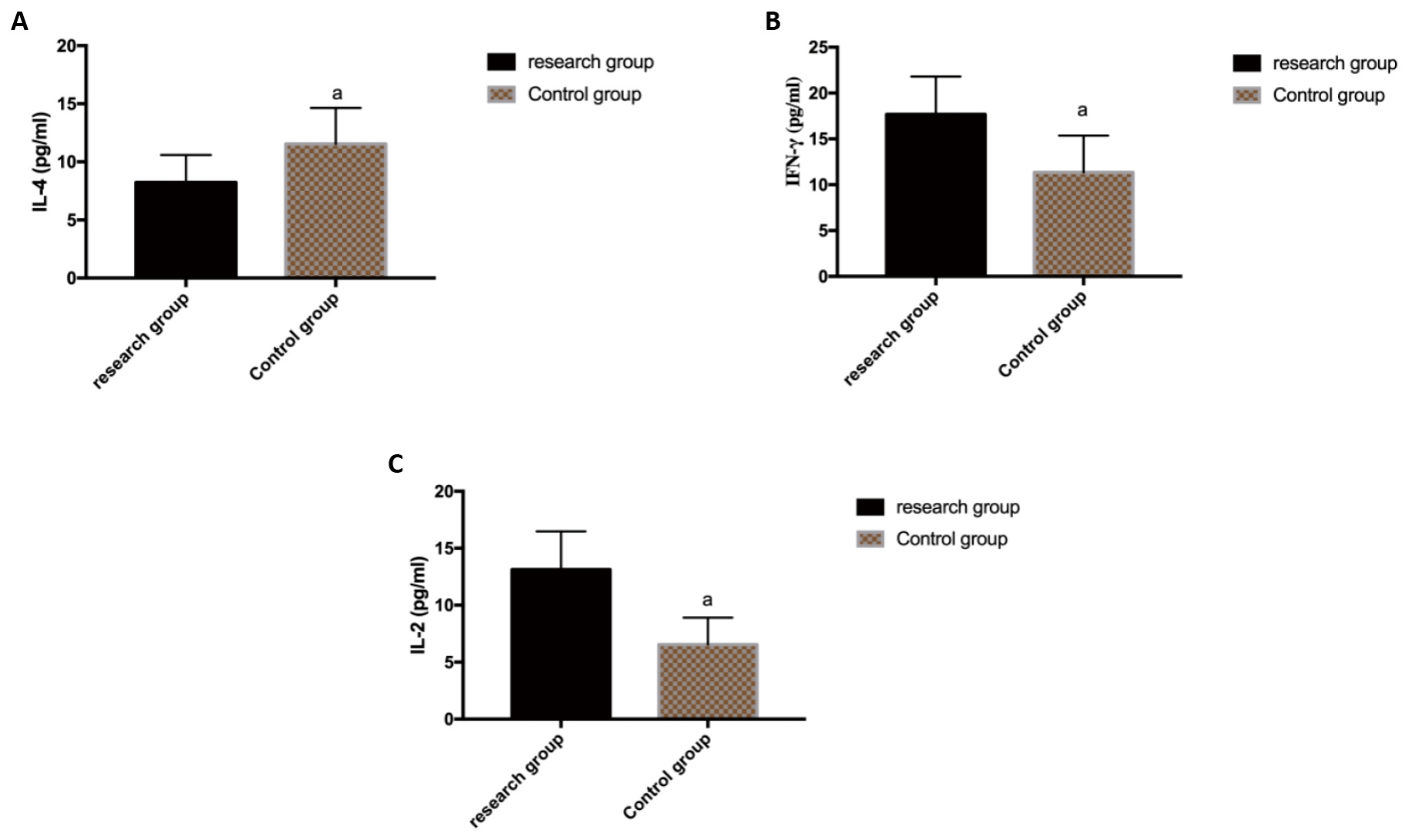
Figure 2. Comparison of IL-4, IFN-γ and IL-2 levels between the CG and the RG after operation. A: Comparison of IL-4 level between the CG and the RG after operation; B: Comparison of IFN-γ level between the CG and the RG after operation; C: Comparison of IL-2 level between the CG and the RG after operation. Note: aP<0.05.
3.5 Comparison of Postoperative CD3+, CD4+ and CD8+ Levels between the CG and the RG
Comparing the postoperative CD3+, CD4+ and CD8+ levels between the CG and the RG, as shown in Figure 3, CD3+, CD4+ levels in the RG were evidently higher than those in the CG (P<0.05), while CD8+ levels in the RG were evidently lower than those in the CG (P<0.05).
|
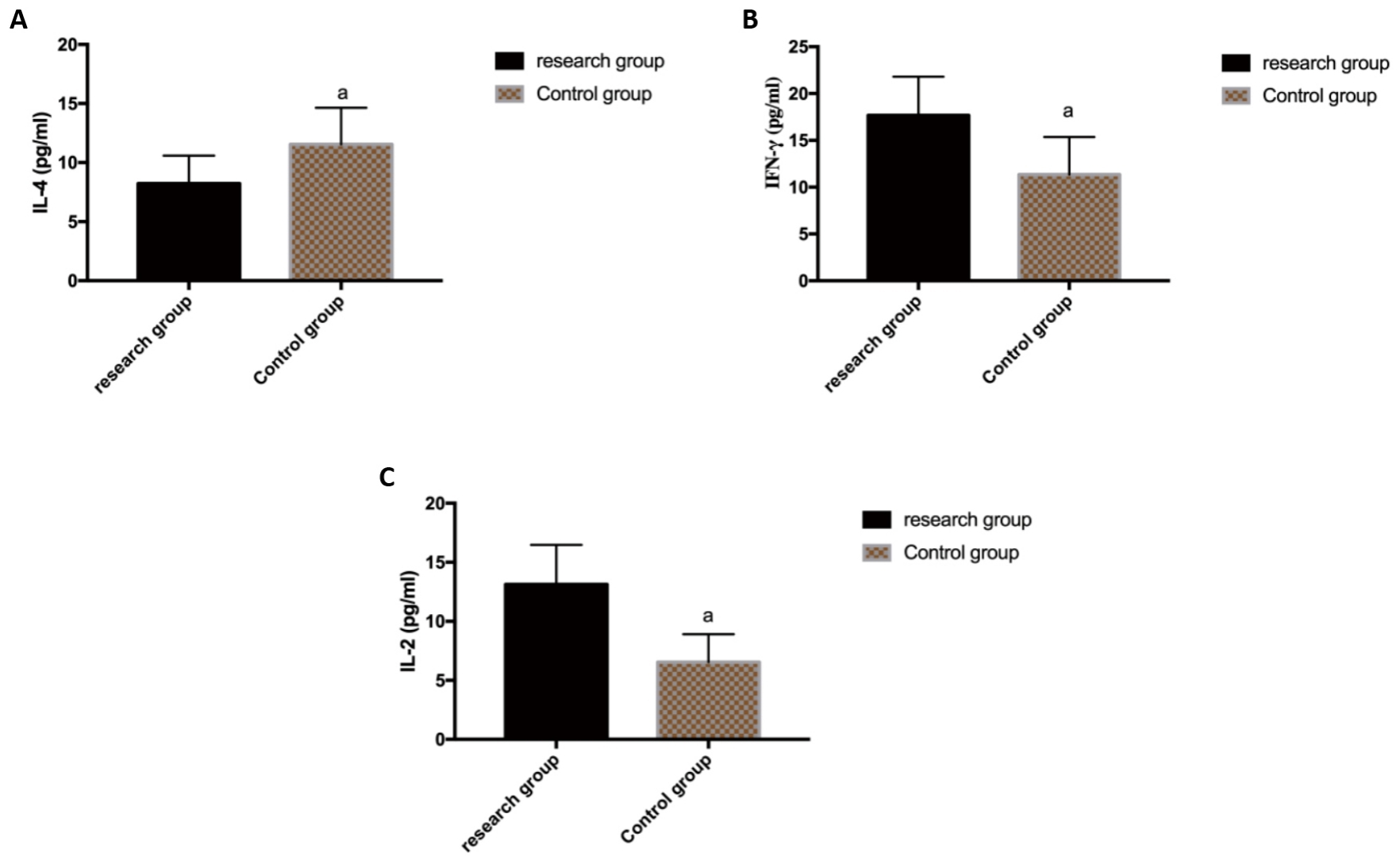
Figure 3. Comparison of postoperative CD3+, CD4+ and CD8+ levels between the CG and the RG. A: Comparison of postoperative CD3+ level between the CG and the RG; B: Comparison of CD4+ level between the CG and the RG after operation; C: Comparison of CD8+ level between the CG and the RG after operation. Note: aP<0.05.
3.6 Psychological Status Scores before and after Intervention
As shown in Figure 4, there was no significant difference in SDS and SAS scores between the CG and the RG before intervention, but after different intervention modes, the scores of SDS and SAS in the RG decreased evidently and were evidently lower than those in the CG (P<0.05).
|
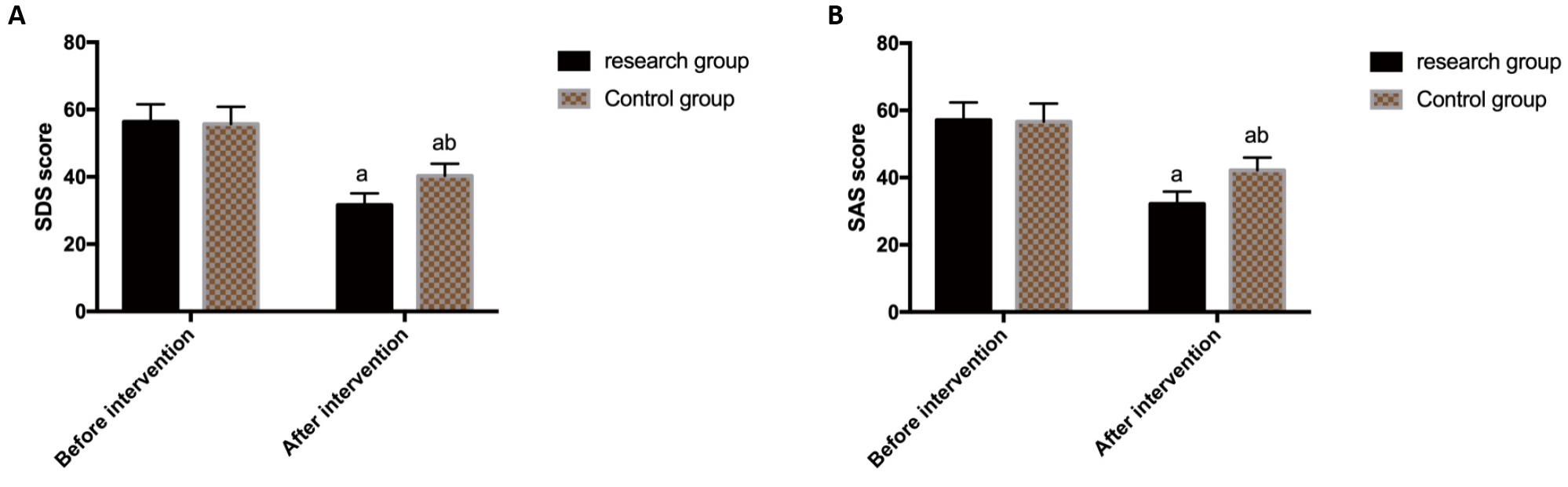
Figure 4. Scores of psychological status before and after treatment. A: Comparison of SDS scores between the CG and the RG before and after treatment; B: Comparison of SAS scores between the CG and the RG before and after treatment. Note: aP<0.05.
3.7 Total Bleeding and Hospital Stay
The total bleeding and hospital stay of the CG and the RG were compared. As shown in Figure 5, the total bleeding and hospital stay of the RG were smaller than those of the CG (P<0.05).
|
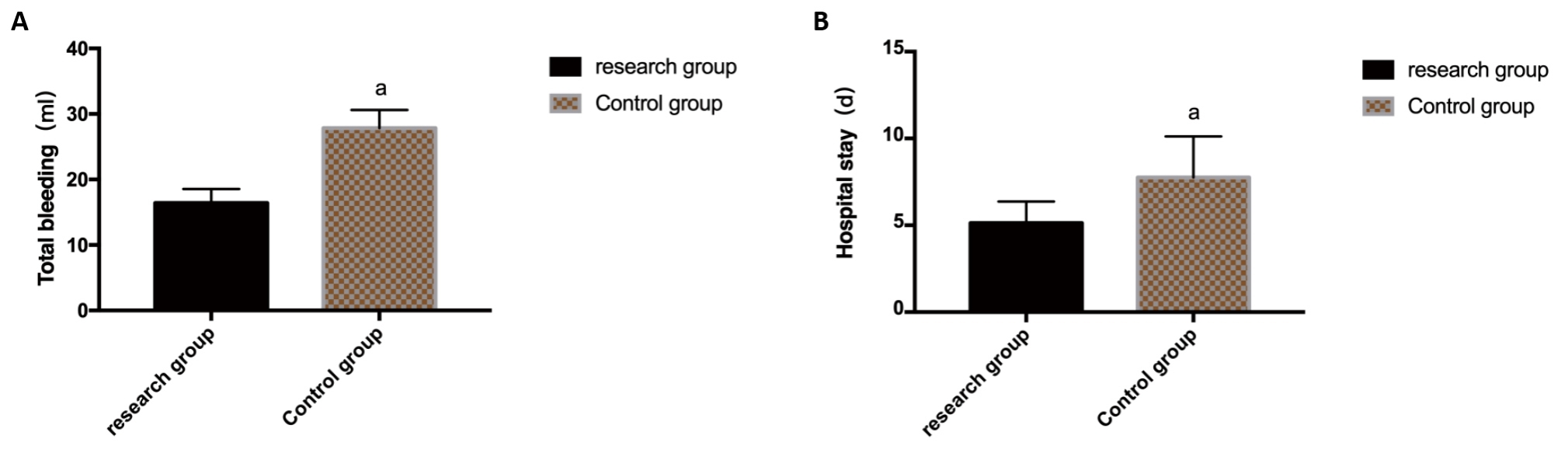
Figure 5. Total bleeding and hospital stay of patients. A: Comparison of total bleeding between the CG and the RG; B: Comparison of hospital stay between the CG and the RG. Note: aP<0.05.
3.8 Quality of Life
Comparing the scores of physiological function, emotional function, coping skills, satisfaction and quality of life between the CG and the RG after treatment, as shown in Figure 6, the scores in the RG after treatment were evidently higher than those in the CG (P<0.05).
|
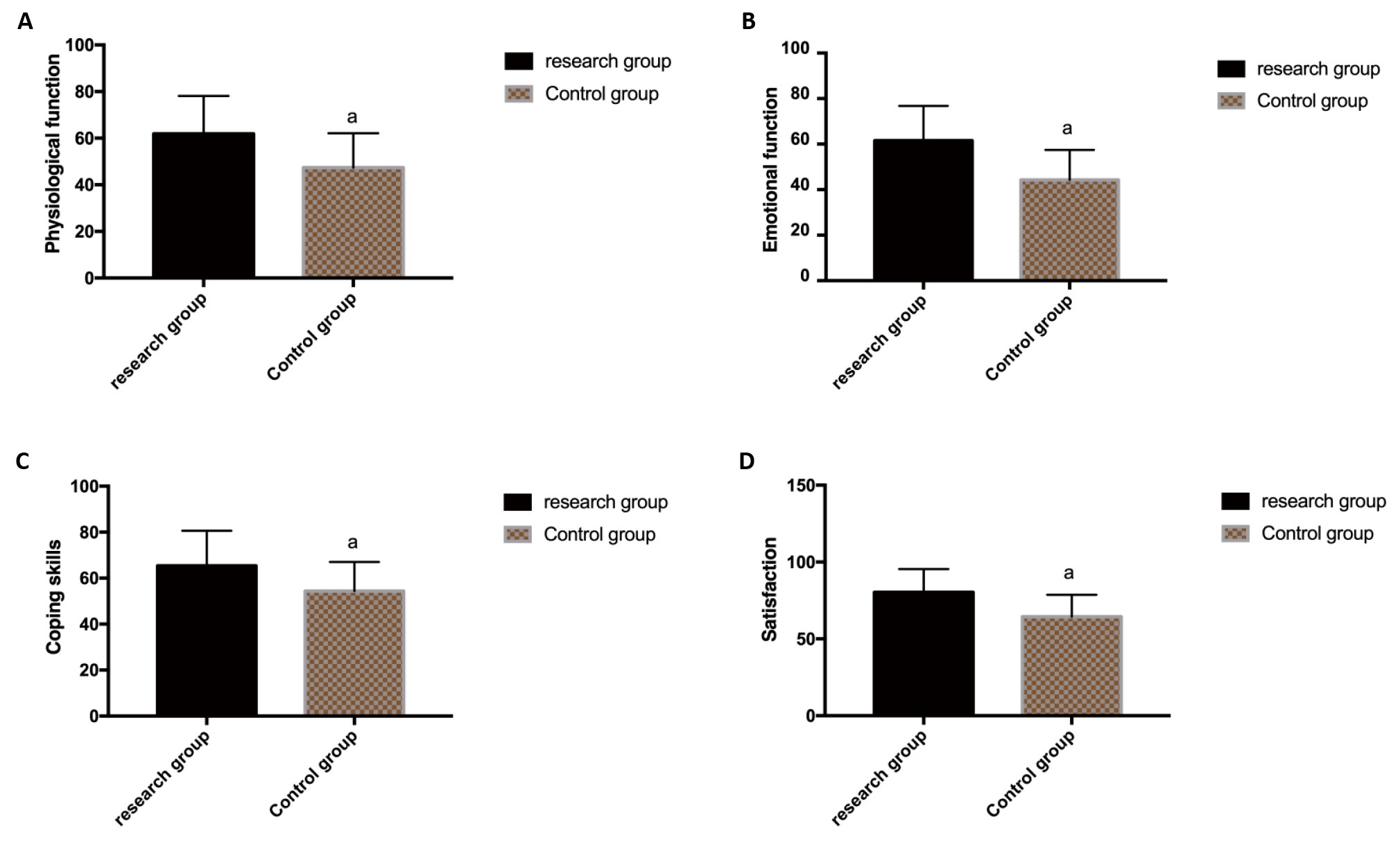
Figure 6. Quality of life of patients. A: Comparison of physiological function between the CG and the RG after treatment; B: Comparison of emotional function between the CG and the RG after treatment; C: Comparison of coping skills between the CG and the RG after treatment; D: Comparison of satisfaction between the CG and the RG after treatment. Note: aP<0.05.
4 Discussion
CIN is a precarcinomaous lesion of cervical carcinoma, which can be classified as CIN 1, CIN 2 or CIN 3 according to histology[15]. In recent ten years, the incidence of CIN is increasing and showing a younger trend[16]. According to the survey data of American pathologist, nearly 1 million women suffer from CIN 1 every year, and 500,000 women are diagnosed with CIN 2 or CIN 3[17]. If not treated in time, it is very likely to develop into invasive cervical carcinoma, threatening the life and health of patients[18]. CIN management has become a public health burden in many parts of the world[19]. At present, LEEP is the main strategy for CIN treatment, and it is also the most commonly used method, with short operation time, convenient operation and low cost[20]. However, with the increasing number of cases in recent years, more and more research reports have pointed out that the incidence of complications of patients after LEEP operation increases and the overall treatment efficiency decreases[21]. We speculate that the wound healing time of patients after LEEP is longer, which easily leads to inflammatory reaction and affects the postoperative recovery of patients. Therefore, Zhikang Capsule, which can clear heat and cool blood, remove blood stasis and stop bleeding, was applied in this research to assist the wound recovery of patients after LEEP operation, and its influence on CIN patients was also observed. The results are as follows:
First of all, the general data of the CG and the RG were compared, such as age, BMI, CIN grade, residence, educational level, family history, smoking history, drinking history, marital status, and nationality. The data showed that there was no statistical difference between the CG and the RG, suggesting that the two groups of patients are comparable. Secondly, the related indexes such as drainage time, bleeding time and wound healing time were compared. The results showed that those of the RG were less than those of the CG, suggesting that Zhikang capsule assisted LEEP intervention could effectively accelerate wound healing and had a positive and effective impact on promoting tissue repair. Zhikang capsule is a traditional Chinese medicine preparation, which contains 14 traditional Chinese medicines, such as resina draconis, rheum officinale, donkey-hide gelatin, dahurian angelica root, and notoginseng, and has the effects of stopping bleeding and removing blood stasis, clearing heat and cooling blood, and promoting granulation and relieving pain[22]. In addition, referring to the relevant data, it was found that Zhikang capsule can alleviate the inflammatory reaction and has better hemostatic effect. Fei et al.[14] revealed that Zhikang capsule could improve colitis induced by dextran sodium sulfate by inhibiting inflammation and apoptosis. This can prove the results of our experiment. Then the incidence of postoperative complications between the CG and the RG was compared. The results showed that the total incidence of postoperative complications in the RG (2.08%) was evidently lower than that in the CG (13.95%). The research suggested that Zhikang capsule assisted with LEEP intervention is safe for CIN patients. It can evidently reduce the complications of application of LEEP operation, such as cervical ectropion, cervical infection, postoperative bleeding, and cervical adhesion, and can promote the curative effect and the recovery. We speculated that its value lies in the fact that Zhikang capsule has an anti-inflammatory effect in wounds. Braber et al.[23] pointed out that Zhikang capsule can effectively hinder intestinal inflammation. This is similar to our experimental results. IL-4, IFN-γ and IL-2 between the CG and the RG were tested and compared to clarify the influence of Zhikang Capsule on inflammatory reaction of CIN patients. The results showed that IL-4 in the RG were evidently lower than those in the CG (P<0.05), while IFN-γ and IL-2 in the RG were evidently higher than those in the CG. Inflammatory factors have unique tolerance mechanism and high sensitivity, and their expression will be affected by trauma and infection, and have immune regulation function[24]. This further confirmed that Zhikang capsule assisted LEEP intervention can obviously eliminate inflammatory reaction of CIN patients. We also compared the postoperative levels of CD3+, CD4+ and CD8+ between the CG and the RG. The results showed that CD3+ and CD4+ in the RG were evidently higher than those in the CG (P<0.05), while CD8+ in the RG were evidently lower than those in the CG. Studies have shown that persistent HPV infection plays an important role in human immune system, and cellular immune function is closely related to the progression of cervical carcinoma[25]. The results indicated that the immune function of CIN patients was evidently improved by the intervention of Zhikang Capsule, suggesting the positive use value of Zhikang capsule for CIN patients. Then, we observed the scores of SDS and SAS before and after intervention. The results showed that the scores of SDS and SAS in the RG were evidently lower than those in the CG after treatment. As the patients' discomfort has been obviously relieved, and their negative psychological state has been improved, so the psychological anxiety has been alleviated, and the mentality has gradually recovered and stabilized. CIN is a precursor lesion of cervical carcinoma[26], which can easily lead to patients' bad moods, such as fear, confusion and irritability. Effective treatment can greatly enhance patients' confidence in their own health, thus the patients could cooperate with the follow-up rehabilitation and the treatment effect can be improved. Finally, we evaluated the total bleeding, hospital stay and quality of life of patients. The data showed that the total bleeding and hospital stay in the RG were smaller than those in the CG, and the scores of physiological function, emotional function, coping skills and satisfaction of patients in the RG were evidently higher than those in the CG, and the quality of life was evidently improved. It is suggested that Zhikang capsule assisted LEEP intervention has great clinical application prospect for CIN.
Due to the limited experimental conditions, there are still some shortcomings in this experiment. The experimental period of this study is short, so we can not evaluate the long-term prognosis of the CG and the RG of patients. At present, there are many treatment measures for CIN in clinic, and it is not excluded that the influence of Zhikang capsule on CIN patients will change when other treatment methods are applied. In the future, we will conduct more in-depth experimental research as soon as possible to expand the sample size and obtain more accurate experimental results for clinical reference.
5 Conclusion
To sum up, Zhikang capsule assisted LEEP surgery intervention in CIN can effectively improve the postoperative recovery rate and reduce the incidence of complications, which is worthy of clinical application.
Acknowledgements
Not applicable.
Conflicts of Interest
The authors declared no conflict of interest.
Author Contribution
Chen C and Zhang H designed this study and wrote the article; Chen C collected the data and performed the statistical analysis; Zhang H revised the papers for important intellectual content; all authors approved the final version.
Abbreviation List
CG, Control group
CIN, Cervical intraepithelial neoplasia
IFN-γ, Interferon-γ
IL-2, Interleukin-2
IL-4, Interleukin-4
LEEP, Loop electrosurgical excision procedure
RG, Research group
References
[1] Small Jr W, Bacon MA, Bajaj A et al. Cervical cancer: A global health crisis. Cancer, 2017; 123: 2404-2412. DOI: 10.1002/cncr.30667
[2] The Cancer Genome Atlas Research Network. Integrated genomic and molecular characterization of cervical cancer.Nature, 2017; 543: 378-384. DOI: 10.1038/nature21386
[3] Arbyn M, Weiderpass E, Bruni L et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health, 2020; 8: e191-e203. DOI: 10.1016/S2214-109X(19)30482-6
[4] Ogilvie GS, Van Niekerk D, Krajden M et al. Effect of screening with primary cervical HPV testing vs cytology testing on high-grade cervical intraepithelial neoplasia at 48 months: the HPV FOCAL randomized clinical trial. JAMA, 2018; 320: 43-52. DOI: 10.1001/jama.2018.7464
[5] Tainio K, Athanasiou A, Tikkinen KAO et al. Clinical course of untreated cervical intraepithelial neoplasia grade 2 under active surveillance: systematic review and meta-analysis. BMJ, 2018; 360: k499. DOI: 10.1136/bmj.k499
[6] Benard VB, Castle PE, Jenison SA et al. Population-Based Incidence Rates of Cervical Intraepithelial Neoplasia in the Human Papillomavirus Vaccine Era. JAMA Oncol, 2017; 3: 833-837. DOI: 10.1001/jamaoncol.2016.3609
[7] Mitra A, Macintyre DA, Ntritsos G et al. The vaginal microbiota associates with the regression of untreated cervical intraepithelial neoplasia 2 lesions. Nat Commun, 2020; 11: 1999. DOI: 10.1038/s41467-020-15856-y
[8] Kelly H, Weiss HA, Benavente Y et al. Association of antiretroviral therapy with high-risk human papillomavirus, cervical intraepithelial neoplasia, and invasive cervical cancer in women living with HIV: a systematic review and meta-analysis. Lancet HIV, 2018; 5: e45-e58. DOI: 10.1016/S2352-3018(17)30149-2
[9] El-Nashar SA, Shazly SA, Hopkins MR et al. Loop Electrosurgical Excision Procedure Instead of Cold-Knife Conization for Cervical Intraepithelial Neoplasia in Women With Unsatisfactory Colposcopic Examinations: A Systematic Review and Meta-Analysis. J Low Genit Tract Dis, 2017; 21: 129-136. DOI: 10.1097/LGT.0000000000000287
[10] Wiik J, Sengpiel V, Kyrgiou M et al. Cervical microbiota in women with cervical intra-epithelial neoplasia, prior to and after local excisional treatment, a Norwegian cohort study. BMC Womens Health, 2019; 19: 30. DOI: 10.1186/s12905-019-0727-0
[11] Hurtado-Roca Y, Becerra-Chauca N, Malca M. Efficacy and safety of cryotherapy, cold cone or thermocoagulation compared to LEEP as a therapy for cervical intraepithelial neoplasia: Systematic review. Rev Saude Publica, 2020; 54: 27. DOI: 10.11606/s1518-8787.2020054001750
[12] Wang XI, Huang F, Zhang S. Loop electrosurgical excision procedure vs. cold knife cone in treatment of cervical intraepithelial neoplasia: review of 447 cases. Ann Clin Lab Sci, 2017; 47: 663-667.
[13] Demirkiran F, Kahramanoglu I, Turan H et al. See and treat strategy by LEEP conization in patients with abnormal cervical cytology. Ginekol Pol, 2017; 88: 349-354. DOI: 10.5603/GP.a2017.0066
[14] Fei L, Xu K. Zhikang Capsule ameliorates dextran sodium sulfate-induced colitis by inhibition of inflammation, apoptosis, oxidative stress and MyD88-dependent TLR4 signaling pathway. J Ethnopharmacol, 2016; 192: 236-247. DOI: 10.1016/j.jep.2016.07.055
[15] Zhang C, Liu Y, Gao W et al. The direct and indirect association of cervical microbiota with the risk of cervical intraepithelial neoplasia. Cancer Med, 2018; 7: 2172-2179. DOI: 10.1002/cam4.1471
[16] Byun JM, Jeong DH, Kim YN et al. Persistent HPV-16 infection leads to recurrence of high-grade cervical intraepithelial neoplasia. Medicine (Baltimore), 2018; 97: e13606. DOI: 10.1097/MD.0000000000013606
[17] Huang J, Qian Z, Gong Y et al. Comprehensive genomic variation profiling of cervical intraepithelial neoplasia and cervical cancer identifies potential targets for cervical cancer early warning. J Med Genet, 2019; 56: 186-194. DOI: 10.1136/jmedgenet-2018-105745
[18] Ebisch RMF, Rutten DWE, IntHout J et al. Long-Lasting Increased Risk of Human Papillomavirus-Related Carcinomas and Premalignancies After Cervical Intraepithelial Neoplasia Grade 3: A Population-Based Cohort Study. J Clin Oncol, 2017; 35: 2542-2550. DOI: 10.1200/JCO.2016.71.4543
[19] Wang H, Ma Y, Li R et al. Associations of Cervicovaginal Lactobacilli With High-Risk Human Papillomavirus Infection, Cervical Intraepithelial Neoplasia, and Cancer: A Systematic Review and Meta-Analysis. J Infect Dis, 2019; 220: 1243-1254. DOI: 10.1093/infdis/jiz325
[20] Barchitta M, Quattrocchi A, Maugeri A et al. LINE-1 hypermethylation in white blood cell DNA is associated with high-grade cervical intraepithelial neoplasia. BMC Cancer, 2017; 17: 601. DOI: 10.1186/s12885-017-3582-0
[21] Zhang H, Lu J, Lu Y et al. Cervical microbiome is altered in cervical intraepithelial neoplasia after loop electrosurgical excision procedure in china. Sci Rep, 2018; 8: 4923. DOI: 10.1038/s41598-018-23389-0
[22] Ahmad TB, Liu L, Kotiw M et al. Review of anti-inflammatory, immune-modulatory and wound healing properties of molluscs. J Ethnopharmacol, 2018; 210: 156-178. DOI: 10.1016/j.jep.2017.08.008
[23] Braber NLV, Nuñez IN, Bohl L et al. Soy genistein administered in soluble chitosan microcapsules maintains antioxidant activity and limits intestinal inflammation. J Nutr Biochem, 2018; 62: 50-58. DOI: 10.1016/j.jnutbio.2018.08.009
[24] Sadri Nahand J, Moghoofei M, Salmaninejad A et al. Pathogenic role of exosomes and microRNAs in HPV-mediated inflammation and cervical cancer: A review. Int J Cancer, 2020; 146: 305-320. DOI: 10.1002/ijc.32688
[25] Van Meir H, Nout RA, Welters MJP et al. Impact of (chemo)radiotherapy on immune cell composition and function in cervical cancer patients. Oncoimmunology, 2017; 6: e1267095. DOI: 10.1080/2162402X.2016.1267095
[26] Chun S, Shin K, Kim KH et al. The Neutrophil-Lymphocyte Ratio Predicts Recurrence of Cervical Intraepithelial Neoplasia. J Cancer, 2017; 8: 2205-2211. DOI: 10.7150/jca.19173
Copyright © 2023 The Author(s). This open-access article is licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, sharing, adaptation, distribution, and reproduction in any medium, provided the original work is properly cited.


